This narrative review aims to elaborate on the aetiopathogenesis, risk factors, clinical features and management of contrast-induced nephropathy and illustrates the potential therapeutic options and management guidelines to prevent the same. Previously called as Contrast Induced Nephropathy (CIN), Contrast-Induced Acute Kidney Injury (CI-AKI) is a type of acute renal failure categorized by unexplained deterioration of kidney function in 24-48 hours post administration of any sort of contrast media. The aetiopathogenesis of this disease is multi-factorial and many patients related and contrast related factors are responsible for its occurrence. Use of various methods like hemofiltration, hemodilation, intravenous calcium administration, low-osmolar contrast agents as well as ischemic preconditioning help to reduce its incidence. Over recent years, intravascular contrast media are commonly being used for therapeutic and diagnostic procedures worldwide, hence there’s been a rise in the incidence of contrast-associated acute kidney injury. It’s the 3rd leading cause of admissions due to acute kidney failure. Till date, there is no definite strategy to prevent CI-AKI, except for careful selection of patients with a meticulous risk/benefit analysis, sufficient intravenous periprocedural and preprocedural hydration with normal saline and sodium bicarbonate, and reducing the amount of contrast agent used. Hence this review was done after an extensive search on Embase, PubMed, GoogleScholar and Cochrane Library database, to identify articles published in the English language that shed ligt on contrast-induced nephropathy using specific keywords like- contrast-induced/contrast-associated nephropathy, acute kidney injury, heamodialysis, osmolality, and renal failure, in order to come to a consensus regarding the most suitable mechanism to prevent CI-AKI for the clinical practitioners. Only publications in English were considered, focusing more on the most recent updates.
INTRODUCTION AND BACKGROUND
Contrast-induced acute kidney injury is characterized by a reduction in kidney function that develops within days after administration of the intravascular iodinated contrast material. Intravascular contrast media are one of the most commonly used materials for therapeutic and diagnostic radiological purposes [1]. This has caused an increase in occurrence of procedure associated Contrast Induced – Acute Kidney Injury (CI-AKI) which was earlier known as Contrast Induced Nephropathy (CIN) [2]. The first report of CI-AKI appeared in the year 1962 [3], after which further research was being done on the potential harmful effects and toxicities of contrast media (CM). Because of the numerous reports of CI-AKI, imaging procedures involving CM are sometimes withheld [4]. Studies have shown that the risk associated with it might be considerably lower than initially estimated [5], even though it is one of the most significant and potentially catastrophic complications in patients undergoing procedures with contrast media. CI-AKI is also the leading cause of acute renal failure in hospitalized patients, ranking third after ischemic and drug-induced injury [6]. A specific estimate of the incidence and prevalence of CI-AKI is needed, owing to the rising number of diagnostic and interventional procedures that use CM. Despite current advancements, the treatment of CI-AKI remains relatively limited and mainly focuses on non-dialytic treatment such as avoidance or discontinuation of nephrotoxic drugs, adjustments of hemodynamic parameters and search for reversible causes [7]. Hence, this review was conducted with the aim to develop appropriate prevention methods and treatment protocols, that areh vital for management of this condition.
MATERIALS AND METHODS
This narrative review was done after an extensive search on Embase, PubMed, Google Scholar and Cochrane Library database, to identify articles published in the English language that shed light on contrast-induced nephropathy using specific keywords like- contrast-induced/contrast-associated nephropathy, acute kidney injury, hemodialysis, osmolality, and renal failure, in order to come to a consensus regarding the most suitable mechanism to prevent CI-AKI for the clinical practitioners. Only publications in English were considered, focusing more on the most recent updates.
REVIEW
DEFINITIONS AND TERMINOLOGIES
Contrast induced nephropathy is defined as an aggravation of the existing renal dysfunction or a recent onset renal disease, after an intravascular contrast injection, when the other renal injury causes have been ruled out. In this review, we used the AKI definition by the Kidney Disease Improving Global Outcomes working group [8]. This definition has also been used in the most recent guidelines by the French nephrology society and the French radiological society, as published in 2021 [9]. As per this definition, either of the following criteria define CA-AKI (Contrast-Associated Acute Kidney Injury) if it occurs in 48 hours after administration of contrast media (CM):
A rise in serum creatinine of more than 26.5 μmol/L (0.3mg/dl);
A rise in serum creatinine of more than ≥ 1.5 times from baseline;
A fall in urine output to less than <0>
Contrast-Associated AKI (CA-AKI) synonymously known as "postcontrast AKI" is a very broad term which refers to the acute kidney injury that occurs post administration of contrast medium, but it may not necessarily because of the contrast material. The term CA-AKI is also applicable to other AKI causing pathological conditions.
"Contrast-induced AKI (CI-AKI)," initially called as "contrast-induced nephropathy (CIN)," is a very specific term which refers to a subset of post-contrast acute kidney injury which is directly linked to the administration of contrast material. In a particluar patient, the link between AKI and contrast exposure can be assessed after thorough history and clinical examination, to ruel out other causes of AKI. If after conducting such an evaluation, no other causal agents (apart from the contrast agent) is identified, then in these situations, it is appropriate to use the term CI-AKI.
The American College of Radiology has introduced new terminologies to clarify the causal relationship between the use of intravascular contrast and the development of acute kidney injury [10]:
Contrast-Associated Acute Kidney Injury (CA-AKI)(Post-Contrast Acute Kidney Injury (PC-AKI): acute kidney injury due to any cause within 48 hours after contrast administration as an association
The American College of Radiology suggests using the term PC-AKI rather than CI-AKI or CIN as the literature points to an association but not causality [10,11].
Post-contrast peak effect on creatinine occurs between 48 and 72 hours [12]:
Relative increase: 50% rise above the baseline
Absolute increase: rise of more than 27 μmol/L
Importantly, CI- AKI needs to be differentiated from post-contrast acute kidney injury without suspected causality between CM administration and AKI. Although it often presents as only transient kidney injury, it may occasionally progress to the significant stage of renal failure that worsens clinical outcome and significantly increases hospital expenditure [13].
PATHOGENESIS OF CI-AKI
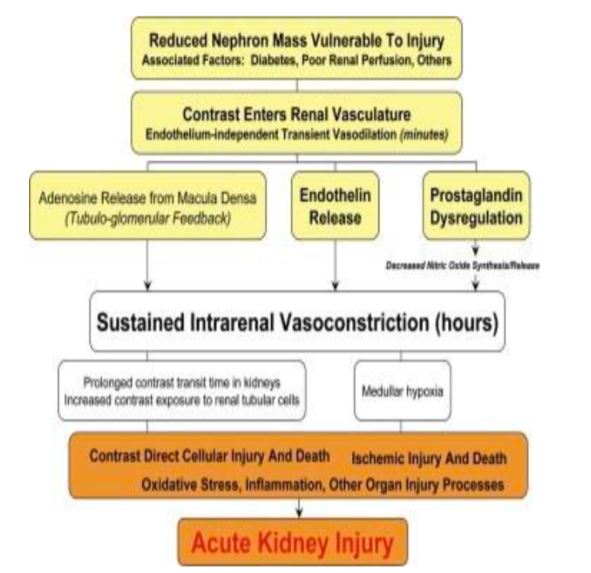
The pathogenesis of CI-AKI is found to be related to multiple factors, and the exact pathogenesis is unknown. It is known to depend on free radicals produced in the acidic environment of the renal medulla, as shown in Figure 1. The hyperosmolar stress that occurs during the use of certain contrasts, stimulates production of reactive oxygen species, causing cytotoxicity and apoptosis of glomeruli and tubular cells [14].
Figure. 1 - Overview of factors involved in the pathogenesis of CI-AKI.(NO= nitric oxide, OH⁻= hydroxyl radical, O⁻₂ Superoxide radical,PaO2 = arterial oxygen pressure.)
Many studies conducted on animals depict that there’s constriction of vasa recta in response to the contrast media, which causes a reduction in the GFR (glomerular filtration rate) and medullary blood flow, reduced oxygen tension, a rise in erythrocyte aggregation and levels of adenosine, endothelin and prostaglandins; leading to dilatation of blood vessels. Furthermore, decreased nitric oxide leads to ischemia in the outer medulla. Immunological etiological factors have also been implicated in its pathogenesis [15].
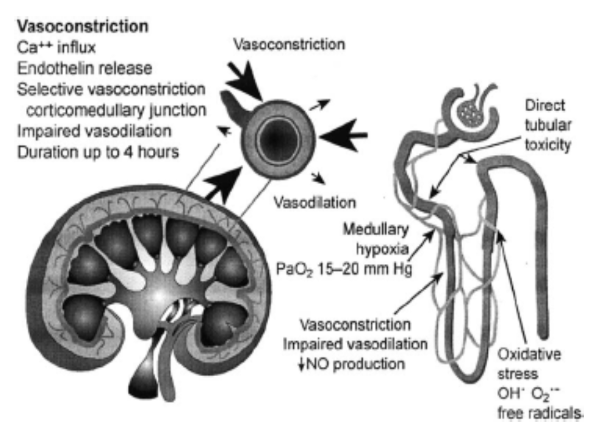
Osmolality of contrast agents has also been proved to have a role in pathogenesis of CI-AKI (Figure 2), as shown by various experimental and clinical studies [16]. Contrast media that have an osmolality higher than that of plasma increase its viscosity, and hence increase the resistance to flow in renal tubules [17]. Intravenous administration of contrast agents has lesser side effects when compared to intra-arterial injections. Studies have shown that the amount of CM required is lesser with intravenous route, and the osmolality of media decreases in circulation before reaching renal system [17].
Figure. 2 - The role of osmolality of the contrast media in the pathogenesis of CI-AKI.
RISK FACTORS FOR CI-AKI
The factors which increase the occurrence of CI-AKI can be categorised as patient related, contrast media related or related to the procedure done.
PATIENT RELATED RISK FACTORS:-
Various patient related factors can be implicated in the occurrence of CI-AKI, like chronic kidney disease (CKD) and diabetes mellitus (DM), which cause reduced vasodilation. Diabetic patients have an alteration of nitric-oxide mediated vasodilatation and there is reduction of renal outer medullary oxygen, alongwith endothelial dysfunction [18]. Diabetic nephropathy and hypertension have been documented as very important risk factors for CI-AKI, due to the intra renal expression of vasoactive substances like nitric oxide.
Angiotensin enzyme inhibitors have a significant effect on reduction of renal function; hence they are also considered as a risk factor in this disease as shown in some studies [19]. Nephrotoxic drugs [20] also make kidneys more prone to the toxic effects of contrast media. Aminoglycosides, sulphanamides, cisplatin and cyclosporin A are a few of the drugs which are associated with CI-AKI, and their effects can be exacerbated if they are combined with furesemide.
PROCEDURE AND CONTRAST MEDIA RELATED RISK FACTORS
High total dose of contrast media, increased osmolality, high viscosity, raised ionic content of the contrast media, intra arterial contrast injection, urgent or emergency procedures, intra-aortic balloon pump use, intervention with bypass graft in case of delayed reperfusion as well as <2>
procedures - all of these factors contribute to an increased risk of developing CI-AKI [21]. A prospective single-centre study conducted at a tertiary care hospital in India showed that the risk of developing CI-AKI is more with intra-arterial iodinated contrast, when compared to intra-venous CM, and the risk is higher among patients’ patients undergoing PCI, and even more so in the South-East Asian population [22,23] Table 1 depicts the various risk factors responsible for CI-AKI.
PATIENT RELATED RISK FACTORS
IODINATED CONTRAST MEDIA
RENAL TOXIC DRUGS
Diabetes mellitus
CM Volume > 100 ml multiple injections
Non-steroid anti-inflammatory drugs
Pre- existing chronic kidney disease
Intra-arterial injection high dose
Chemotherapy drugs- cyclosporin, platin groups
Old age
Short time interval between injections (<72>
Calcineurin inhibitors
Decreased serum albumin - less than < 35>
High Osmolality and high viscosity contrast Injected
Table 1- Table showing various risk factors for CI-AKI.
STRATEGIES FOR PREVENTION OF CI-AKI
NON-PHARMACOLOGICAL PREVENTION STRATEGIES OF CI-AKI
SELECTION OF CONTRAST AGENT AND DOSE REDUCTION
According to the published data on prevention of CI-AKI, minimizing the use of iodinated contrast agents and using low or iso-osmolar CM (contrast media) agents appears to be of greatest importance. These recommendations are included in the recent guidelines by both- the European Society of Cardiology [24] and the American College of Cardiology [25]. Currently, the most commonly used contrast media are the non-ionic low-osmolar agents, especially iodixanol. Low-osmolar CM are found to be superior to iso-osmolar CM [26].
HYDRATION
Hydration is the cornerstone of preventive care as it can reduce the tubular content and consistency of the contrast medium; it can reduce the stimulation of RAAS (renin–angioten- sin–aldosterone system); it inhibits diuretic hormone synthesis, and minimizes volume depletion and synthesis of prostacyclins, thus reducing renal perfusion and causing medullary hypoxia [27]. Oral fluid intake increases diuresis via inhibition of vasopressin release, and in contrast, normal saline causes suppression of RAAS, thus slowing renal responses to intravenous isotonic saline administration, but it also provides long-term renal protection. Eisenberg et al. conducted a prospective study and reported that renal failure following large angiography could be prevented using the fluid intake procedure in response to the reported rate of post-angiographic acute renal failure of 12% [28].
INTRACELLULAR CALCIUM OVERLOAD
Intra-cellular calcium plays an important role in causing ischemic cell injury, resulting in CI-AKI. A rise in intracellular calcium can cause vasoconstriction in the renal circulation, resulting in necrosis and apoptosis of epithelial cells. Hence, calcium channel blockers can be administered for thier preventive effect on CI-AKI. However, the use of calcium channel blockers has led to spurious findings, in that some authors contend that it offers protection [29,30], while others claim that it offers no advantage [31,32].
EFFECTS OF ISCHEMIC PRECONDITIONING
Ischemic preconditioning is a non-invasive and non-pharmacological procedure which was first described among dogs in the year 1986 and among humans in 1993. This technique was developed to “prime” the cells against ischemic trauma that might occur in the future, and it involves a sequence of ischemia and reperfusion, before the ischemia sets in. In the absence of oxygen and nutrition, anaerobic glycolysis occurs and there is suppression of oxidative phosphorylation. Slowing down of cellular metabolism after reperfusion and the oxidative burst, collectively cause the release of high levels of reactive oxygen species and many pro-inflammatory cytokines; which result in cellular damage [33].
Many studies have examined if remote ischemic preconditioning (RIPC) can have a protective effect on the renal system. A meta-analysis by Gen et al. showed that RIPC can reduce risk of CI-AKI in patients undergoing PCI [34].
B. PHARMACOLOGICAL PREVENTION STRATEGIES
N-ACETYL CYSTEINE (NAC)
For twenty years, many clinical trials have been investigating acetylcysteine in prevention of CI-AKI, and their results are highly inconclusive. The probable mechanism by which NAC may reduce vasoconstriction and oxygen free radical generation after contrast media exposure is by direct vasodilation of kidney vessels and reducing endothelial cell dysfunction, thereby contributing to improved renal hemodynamics [2]. But some studies show conflicting evidence regarding its efficacy. In the PRESERVE trial, oral acetylcysteine was administered at a dose of 1200 mg twice daily for 5 days, beginning on the day of angiography [35]. When compared to a placebo, acetylcysteine did not cause reduction in mortality rates or in the rates of renal derangement at 90 days. Also, it did not reduce the requirement for dialysis (4.6% with acetylcysteine and 4.5% with placebo; odds ratio, 1.02; 95% CI, 0.78 to 1.33) and neither did it reduce the rates of CI-AKI (9.1% and 8.7%, respectively; odds ratio, 1.06; 95% CI, 0.87 to 1.28). These findings imply that routine administration of N-acetylcysteine may not be as helpful in prevention of CI-AKI, or in the prevention of long-term adverse events after angiographic procedures.
STATINS
Numerous studies have been done on statins to identify them as potential agents in prevention of CI-AKI among patients undergoing PCI, attributing to their beneficial effect on oxidative stress and endothelial function, as well as their anti-inflammatory and anti-oxidant properties [2]. This is a very favourable approach as majority of the patients who undergo PCI are already taking these drugs. The PRATO-ACS (Protective Effect of Rosuvastatin and Antiplatelet Therapy on Contrast-Induced Acute Kidney Injury and Myocardial Damage in Patients with Acute Coronary Syndrome) trial [36] showed a significant reduction in rates of acute kidney injury and 30-day cardiovascular and renal events after PCI, in patients treated with high-dose rosuvastatin (40-mg loading dose on admission followed by a maintenance dose of 20 mg per day) as compared to patients who didn’t receive tretatment with statins. However, the PROMISS (Prevention of Radiocontrast Medium–Induced Nephropathy Using Short-Term High-Dose Simvastatin in Patients with Renal Insufficiency Undergoing Coronary Angiography) trial [37] failed to show a difference between simvastatin and placebo with respect to a primary end point, as per the mean peak increase in the plasma creatinine levels within 48 hours after angiography, in patients with chronic kidney disease.
HEMODIALYSIS AND HEMOFILTRATION
The removal of X-ray contrast agent by hemofiltration or hemodialysis immediately after X-ray therapy was suggested by Schindler et al. [38]. Contrast agents (iopromide or iomeprol), high-flux hemodialysis and hemofiltration have been found to successfully remove the contrast agents but do not prevent CI-AKI in patients with CKD [39]. In a study by Vogt et al, prophylactic hemodialysis was tested to see if it can prevent CI-AKI, immediately following the delivery of a hypotonic contrast agent, in patients with renal impairment i.e. baseline serum creatinine level > 2.3 mg/dl [40]. Monitoring of kidney function was done prior to and for six days post contrast administration. The authors of this study concluded that incorporating the use of hemodialysis as preventive measure did not decrease the incidence of CI-AKI.
Table 2 gives a brief outline of the various studies reporting preventive strategies for CI-AKI.
NON-PHARMACOLOGICAL STRATEGIES
PHARMACOLOGICAL STRATEGIES
SELECTION OF CM AND DOSE REDUCTION
Low volume and low-osmolar agents contrast media preferred (CM)
Suggested by- European Society of Cardiology [33] and the American College of Cardiology [34].
N-ACETYLCYSTEINE
Decrease free radical oxygen and reduces endothelial dysfunction
Inconclusive results by many studies and trials- PRESERVE TRIAL [48]
HYDRATION
Suppression of RAAS; normal saline used along with sodium bicarbonate or use of only sodium chloride
Eisenberg et al [39]
STATINS
Anti-inflammatory and anti-oxidant properties.
Premising results by PRATO-ACS [49] trial, but inconclusive results by PROMISS trial [50].
INTRACELLULAR CALCIUM OVERLOAD
Use of CCBs (Calcium Channel Blockers) to increase intra-renall calcium content
Many authors have contrasting opinions regarding this modality [40-45]
HEMODIALYSIS
AND HEMOFILTRATION
Helps in removal of contrast agent but does not have any preventative effect on CA-AKI
First suggested by Schindler et al [51], No beneficial result in a study by Vogt et al [53].
ISCHEMIC PRECONDITIONING
Sequence of ischemia/reperfusion gives rise to increased anaerobic glycolysis and reduced oxidative phosphorylation
Suggested by Wever et al [46]and Dang et al [47]
Table 2- Studies Reporting Strategies for Prevention of CI-AKI.
GUIDELINES USED FOR PREVENTION OF CI-AKI
According to the Consensus Guidelines [41] for the Prevention of Contrast-Induced Nephropathy by the Canadian Association of Radiologists, serum creatinine is not a reliable measure of renal function. Rather, the most reliable method to decrease the incidence of CI-AKI is use of eGFR for assigning risk levels and to apply preventive measures.
When GFR is less than 60, guidelines for all CI-AKI patients are: -
• Avoid iodinated contrast media as much as possible
• Avoid nephrotoxic medications 48 hours prior to CM administration
• Use of iso- or low-osmolar CM and avoid using high osmolar CM
• Reduce the amount of CM used and avoid repetition of the procedure within 72 hours
• Consider N-acetylcysteine (NAC) in patients having CI-AKI
When GFR is between 30–60, guidelines for all CI-AKI patients are: -
Avoid volume contraction in patients
Provide intra-venous or oral fluids
Provide a GFR follow-up 48 hours post contrast administration
When GFR is 30, the specific guidelines for patients are: -
Intra-venous fluid administration (sodium bicarbonate or normal saline) for volume expansion
Provide a GFR follow-up 48 hours post CM administration
As per the guidelines published by ESUR Contrast Media Safety Committee [42], only the patients having eGFR of less than 45 ml/min/1.73 m2 are at a high risk of CI-AKI before administration of intravenous (IV) iodinated CM. Moreover, they also found that the risk of CI-AKI is less after IV administration rather than intra-arterial CM; at similar doses. This committee also proposed that either normal saline or sodium bicarbonate must be administered for volume expansion and to prevent CI-AKI.
CONCLUSIONS
CI-AKI is an iatrogenic condition which is commonly seen among high-risk patients undergoing radiological procedures with an intra-arterial or an intravenous contrast dye injection. Till date, there is no definite strategy to prevent CI-AKI, except for careful patient selection and a meticulous risk/benefit analysis, sufficient intervenus per procédural and preprocedural hydration with saline and sodium bicarbonate, and reducing the quantity of contrast agent used. The preventive role of N-acetylcysteine is not very well proven. Even though an absolutely harmless contrast material does not exist, iso-osmolar or low osmolar contrastes are known to have higher safety in terms of nephrotoxicity when compared to high osmolar agents, and this is highly recommended by the recent guidelines. Preventive hemofiltración and hydration 6 hours prior to a contrast procedure should be considered in extremely high-risk subjects, although more extensive research is needed to validate this finding. Other therapies, like ischemic preconditioning and intravenous calcium administration can be considered, but further data is required before adopting the same for prevention of CI-AKI.
DATA AVAILABILITY STATEMENT
Data has been collected from the below mentioned references.
References
Mohammed NM, Mahfouz A, Achkar K, Rafie IM, Hajar R. Contrast-induced Nephropathy. Heart Views. 2013 Jul;14(3):106-16. View
at PublisherView
at Google Scholar
Ali A, Bhan C, Malik M, et al. (September 11, 2018) The Prevention and Management of Contrast-induced Acute Kidney Injury: A Mini-review of the Literature. Cureus 10(9): e3284. View
at PublisherView
at Google Scholar
BERLYNE N, BERLYNE GM. Acute renal failure following intravenous pyelography with hypaque. Acta Med Scand. 1962 Jan;171:39-41. View
at PublisherView
at Google Scholar
Chertow G. ‘Renalism’: inappropriately low rates of coronary angiography in elderly individuals with renal insufficiency. J Am Soc Nephrol. (2004) 15:2462–8. View
at PublisherView
at Google Scholar
Kashani K, Levin A, Schetz M. Contrast-associated acute kidney injury is a myth: we are not sure. Intensive Care Med. (2018) 44:110–4. View
at PublisherView
at Google Scholar
Waikar S, Liu K, Chertow G. Diagnosis, epidemiology and outcomes of acute kidney injury. Clin J Am Soc Nephrol. (2008) 3:844–61. View
at PublisherView
at Google Scholar
Kellum J, Romagnani P, Ashuntantang G, Ronco C, Zarbock A, Anders H, et al. Acute kidney injury. Nat Rev Dis Prim. (2021) 7:52. View
at PublisherView
at Google Scholar
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–138. View
at PublisherView
at Google Scholar
de Laforcade L, Bobot M, Bellin M, Clément O, Grangé S, Grenier N, et al. Kidney and contrast media: common viewpoint of the french nephrology societies (SFNDT, FIRN, CJN) and the french radiological society (SFR) following ESUR guidelines. Diagn Interv Imaging. (2021) 102:131–9. View
at PublisherView
at Google Scholar
American College of Radiology Manual on Contrast Media, version 10.3. https://www.acr.org/Clinical-Resources/Contrast-Manual, accessed 25 April 2018 View
at PublisherView
at Google Scholar
Davenport M, Perazella M, Yee J et al. Use of Intravenous Iodinated Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation. Radiology. 2020;294(3):660-8. View
at PublisherView
at Google Scholar
Mehran R, Dangas GD, Weisbord SD. Contrast-Associated Acute Kidney Injury. New England Journal of Medicine. 2019. 146-2155. 380(22) View
at PublisherView
at Google Scholar
Sůva M, Kala P, Poloczek M, Kaňovský J, Štípal R, Radvan M, Hlasensky J, Hudec M, Brázdil V, Řehǒrová J (2022) Contrast-induced acute kidney injury and its contemporary prevention. Front. Cardiovasc. Med. 9:1073072. View
at PublisherView
at Google Scholar
Shams E, Mayrovitz H N (May 04, 2021) Contrast-Induced Nephropathy: A Review of Mechanisms and Risks. Cureus 13(5): e14842. View
at PublisherView
at Google Scholar
Koch JA, Plum J, et al. PGE1 Study Group, Prostaglandin E1: a new agent for the prevention of renal dysfunction in high risk patients caused by radiocontrast media?, Nephrology Dialysis Transplantation, Volume 15, (1), Jan 2000, 43–49. View
at PublisherView
at Google Scholar
Persson PB, Hansell P, Liss P. Pathophysiology of contrast medium-induced nephropathy. Int Soc Nephrol. 2005;68:14-22. View
at PublisherView
at Google Scholar
Bartholomew BA, Harjai KJ, Dukkipati S, et al. Impact of nephropathy after percutaneous coronary intervention and a method for risk stratification. Am J Cardiol 2004;93:1515–1519. View
at PublisherView
at Google Scholar
Heyman SN, Rosenberger C, Rosen S. Regional alterations in renal haemodynamics and oxygenation: a role in contrast medium-induced nephropathy. Nephrol Dial Transplant Suppl 2005;20:6–11. View
at PublisherView
at Google Scholar
Jo SH, Youn TJ, Park JS, Koo BK, Kang HJ. Iodixanol is less nephrotoxic than ioxaglate in patients with renal insufficiency after coronary angiography [abstract]. J Am Coll Cardiol. 2005;45(suppl 1):A31. View
at PublisherView
at Google Scholar
Solomon R. The role of osmolality in the incidence of contrast-induced nephropathy: a systematic review of angiographic contrast media in high risk patients. Kidney Int. 2005;68:2256–2263. View
at PublisherView
at Google Scholar
Moideen A, Sajgure A, Dighe T, Bale C. SUN-001 A COMPARATIVE STUDY ON THE INCIDENCE OF CONTRAST INDUCED NEPHROPATHY AND ITS RISK FACTORS FOLLOWING INTRA-ARTERIAL VERSUS INTRAVENOUS CONTRAST ADMINISTRATION. Kidney International Reports 2020. 5(3) suppl S205. View
at PublisherView
at Google Scholar
Hassan Z, Kumari U, Wasim U, et al. (February 22, 2024) An Investigation of Contrast-Induced Acute Kidney Injury in Patients Undergoing Percutaneous Coronary Intervention: A Cross-Sectional Study From Pakistan. Cureus 16(2): e54726. View
at PublisherView
at Google Scholar
Neumann F, Sousa-Uva M, Ahlsson A, Alfonso F, Banning A, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. (2019) 40:87–165. View
at PublisherView
at Google Scholar
Lawton J, Tamis-Holland J, Bangalore S, Bates E, Beckie T, Bischoff J, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. (2022) 145:e18–114. View
at PublisherView
at Google Scholar
Poh W, Omar M, Tan H. Predictive factors for contrast-induced acute kidney injury in high-risk patients given N-acetylcysteine prophylaxis. Ann Saudi Med. (2018) 38:269–76. View
at PublisherView
at Google Scholar
Eisenberg RL, Bank WO, Hedgock MW. Renal failure after major angiography can be avoided with hydration. Am J Roentgenol. 1981;36:859–61. View
at PublisherView
at Google Scholar
Toruan M, Pranata R, Setianto B, Haryana S. The role of microRNA in contrast-induced nephropathy: a scoping review and meta-analysis. Biomed Res Int. (2020) 2020:1–6. View
at PublisherView
at Google Scholar
Cheng W, Li X, Xiao Y, Duan S. Non-coding RNA-associated ceRNA networks in a new contrast-induced acute kidney injury rat model. Mol Ther Nucleic Acids. (2019) 17:102–12. View
at PublisherView
at Google Scholar
Sun Q, Kang Z, Li Z, Xun M. Urinary NGAL, IGFBP-7, and TIMP-2: novel biomarkers to predict contrast medium-induced acute kidney injury in children. Ren Fail. (2022) 44:1201–6. View
at PublisherView
at Google Scholar
Sůva M, Kala P, Poloczek M, Kaňovský J, Štípal R, Radvan M, Hlasensky J, Hudec M, Brázdil V, Řehǒrová J (2022) Contrast-induced acute kidney injury and its contemporary prevention. Front. Cardiovasc. Med. 9:1073072. View
at PublisherView
at Google Scholar
Igarashi G, Iino K, Watanabe H, Ito H. Remote ischemic pre-conditioning alleviates contrast-induced acute kidney injury in patients with moderate chronic kidney disease. Circ J. 2013;77(12):3037-44. doi: 10.1253/circj.cj-13-0171. View
at PublisherView
at Google Scholar
Leoncini M, Toso A, Maioli M, et al. Early high-dose rosuvastatin and cardio-protection in the protective effect of rosuvastatin and antiplatelet therapy on contrast-induced acute kidney injury and myocardial damage in patients with acute coronary syndrome (PRATO-ACS) study. Am Heart J 2014;168:792-7. View
at PublisherView
at Google Scholar
Jo SH, Koo BK, Park JS, et al. Prevention of radiocontrast medium-induced nephropathy using short-term high-dose simvastatin in patients with renal insufficiency undergoing coronary angiography (PROMISS) trial — a randomized controlled study. Am Heart J 2008;155(3):499. e1-8. View
at PublisherView
at Google Scholar
Schindler R, Stahl C, Venz S, Ludat K, Krause W, Frei U. Removal of contrast media by different extracorporeal treatments. Nephrol Dial Transplant. 2001;16(7):1471–4. View
at PublisherView
at Google Scholar
Lehnert T, Keller E, Gondolf K, Schaffner T, Pavenst H, Schollmeyer P. Effect of hemodialysis after contrast medium administration in patients with renal insufficiency. Nephrol Dial Transplant. 1998;13(2):358–62. View
at PublisherView
at Google Scholar
Vogt B, Ferrari P, Schonholzer C. Prophylactic hemodialysis after radio contrast media in patients with renal insufficiency is potentially harmful. Am J Med. 2001;111(9):692–8. View
at PublisherView
at Google Scholar
Benko A, Fraser-Hill M, Magner P, Capusten B, Barrett B, Myers A, Owen RJ, Canadian Association of Radiologists. Canadian Association of Radiologists: consensus guidelines for the prevention of contrast-induced nephropathy. Can Assoc Radiol J. 2007;58(2):79–87. View
at PublisherView
at Google Scholar
Stacul F, van der Molen AJ, Reimer P, Webb JA, Thomsen HS, Morcos SK, Almén T, Aspelin P, Bellin MF, Clement O, Heinz-Peer G. Contrast media safety of urogenital radiology (ESUR). Contrast induced nephropathy: updated ESUR contrast media. Eur Radiol. 2011;21(12):2527–41. View
at PublisherView
at Google Scholar
"ScienceHood Publishing exceeded our expectations with their seamless execution and professionalism. Their team ensured timely communication, high-quality production, and attention to detail throughout the process. They transformed our vision into reality, delivering exceptional results. We highly recommend them for their efficiency, expertise, and commitment to excellence in publishing."
Lara Simmons
"ScienceHood Publishing surpassed our expectations with their professionalism, timely communication, and exceptional attention to detail. They transformed our vision into reality with outstanding results. We highly recommend them for their expertise and commitment to excellence."
Shippora Smith
"Publishing in this journal gave me the opportunity to involve Bioinformatics, which is a cutting-edge field with so much potential, into my previous research on Optogenetics and Artificial Intelligence. This experience helped me better understand how closely interconnected STEM fields truly are, and how many opportunities exist for interdisciplinary collaboration to allow them to work together and, once again, change the world, as science has always done"
Tomas Hadi Acosta Aguilera
"Dear editors,
It has also been a real pleasure working with you on the publication of our article. Your patience, understanding, and prompt responses whenever we needed them have been a great help to us in this joint endeavour."


 :
© 2025 Adel Moideen. This open-access article is distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
:
© 2025 Adel Moideen. This open-access article is distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.