Background: Guinea is one of the countries where maternal mortality remains high (550 deaths per 100,000 live births). Despite progress made in improving women's sexual and reproductive health, access to and use of health services remain low, partly due to constraints related to women's autonomy.
Aim: This study was aimed to determine the factors associated with women's decision-making autonomy in healthcare in Guinea
Methods: We analyzed data from 3,880 married women aged 15 to 49 from the 2018 DHS. A simple binary logistic regression model was used to analyze the factors associated with women's decision-making autonomy in healthcare.
Results: Of the 3,880 married women included in the study, only 10.3% were able to make decisions about using health services on their own. Women's decision-making autonomy was significantly associated with employment status and contraceptive use. Women who worked and those who used contraception were approximately twice and three times more likely to make decisions about their healthcare on their own than their counterparts (AOR= 1.7; CI: (1.57 - 1.75) and AOR= 3.1 (2.31 - 4.17) respectively).
Conclusion: Only 10.3% of women could decide on their own to use a health service. These findings will help policymakers develop appropriate interventions to improve women's empowerment.
INTRODUCTION
Despite efforts to improve maternal health, maternal mortality remains a global public health challenge, particularly in low- and middle-income countries. According to the World Health Organization (WHO), around 229,000 maternal deaths worldwide in 2017 were due to complications of unwanted pregnancy and unsafe childbirth. Sub-Saharan Africa and South Asia were the most affected regions (66% and 20%) [1].
In Guinea, despite the government's efforts to improve maternal health, maternal mortality remains very high at 550 deaths per 100,000 live births according to the Demographic and Health Survey (EDS V 2018) [2]. Substantial progress is essential to combat all causes of maternal death in order to achieve the Sustainable Development Goals (SDGs) by 2023. Indeed, a strong decision-making capacity amongst women in terms of healthcare contributes to reducing maternal mortality [3,4]. Women's empowerment refers to their ability to make decisions about their own health and that of their children, without having to seek advice from a third party [5,6]. Women’s participation in the health care decision-making process is an indicator that contributes both to the improvement of maternal and child health and to the development of communities in several countries [7-9]. However, in some countries, women have little say in controlling their finances and lack a certain freedom to act [10]. Often shrouded by customs and religious traditions, women are denied the right to decide their own lives [10,11]. They would like to have the opportunity to fully participate in healthcare planning and even the ability to understand and apply the best available evidence to their individual situation [12].
Evidence has shown that women's limited autonomy prevents them from using maternal health care, such as antenatal consultations/care, delivery in a health facility and postnatal care [13]. The same applies to child mortality. In Nepal, for example, the infant mortality rate was high among women who were not involved in healthcare decision-making [14]. The trend in women's autonomy in healthcare decision-making fell slightly from 18.7% to 17.2
METHODOLOGY
Study setting Guinea is located in the western part of the African continent. Administratively, the country is divided into eight administrative regions, with Conakry as capital city. The administrative regions are further subdivided into 33 prefectures. The country’s socio-economic situation is marked by persistent poverty and food insecurity, which have an impact on the quality of the overall population’s diet. According to the results of the Global Analysis of Vulnerability, Food Security and Nutrition (GAVFSN), around 55.2% of the population lives below the poverty line, which was estimated at 13,717 Guinean francs (GNF)/person/day (or EUR 1.1) in 2019 [17]. In terms of human development, the country ranked 182nd out of 189 countries according to the United Nations Development Program (UNDP) report [18].
Method
Study design This was a secondary analysis of the data from the 2018 Guinea Demographic and Health Survey (DHS), which is a cross-sectional survey. Methodology for data collection and reports are available and accessible on the DHS program website. For this study, data from the individual women questionnaire were used.
Study population and sampling We considered all women aged 15 to 49 from the individual women questionnaire as the study population. The number of women interviewed was 10,506. The analysis focused on women's socio-demographic characteristics, household socio-economic conditions and women's participation in decision-making about their healthcare. Of a total of 7,812 married women, 3,880 were eligible for analysis, after excluding unmarried women, those who did not have a partner or those for whom information on marital status was not available.
Study variables The dependent variable is women's autonomy in healthcare decision-making, which was measured based on women's answer to the question "Who usually decides about your healthcare?". Answers of this dependent variable were coded as (1) independently, (2) with husband/other. This is due to the fact that an individual is autonomous when he/she can act under his/her own direction, i.e. carry out actions concerning himself without the agreement of a third party [15,19]. Thus, women who decide independently about their healthcare were considered to be autonomous in healthcare decision-making.
Independent variables The explanatory variables in this study were classified according to participants’ sociodemographic characteristics (Table 1).
Variables
Modalities
Woman's age
0= 15 and 24 years
1= 25 to 34 years
2= 35 to 49 years
Woman's education level
0= None
1= Primary
2= Secondary/higher
Husband's education level
0= None
1 = Primary
2 = Secondary/higher
Women's current working status
1= Yes
2= No
Husband's occupation
0= No occupation
1= Public/private service
2= Tradesman
3= Farmer
4= Daily labourer
Number of children under 5 years old
0=< 3>
1= ≥ 3 children
Distance from health facility
0= A real problem
1= Not a problem
Women’s socio-economic status
0= Poorest
1= Poorer
2= Middle
3= Richer
4= Richest
Number of ANCs attended
0= < 4>
1= ≥ 4 ANCs
Postnatal consultation
0= No
1= Yes
Place of residence
0= Urban
1= Rural
Region
0= Boké
1= Conakry
2= Faranah
3= Kankan
4= Kindia
5= Labé
6= Mamou
7=Nzérékoré
Table 1: List of study variables
Data processing and analysis
Stata software version 16.1 was used for data cleaning, processing and analysis. A descriptive statistical analysis was carried out. Proportions were calculated for categorical variables; means and standard deviation were calculated for continuous variables. The proportion of women's autonomy in healthcare decision-making was reported on the general population and according to socio-demographic characteristics. Chi-square was applied to assess the association between categorical variables with a significance level of 5%. All estimates were weighted according to the selection probabilities of each participant.
A binary logistic regression model was used to determine the factors associated with women's autonomy in healthcare decision-making.
Crude and adjusted odds ratio (ORs) with their 95% confidence intervals (CIs) were calculated.
The final model was obtained using the following method:
-The variables to be included in the multivariate analysis were determined by a univariate analysis between the dependent variable and all the explanatory variables, and the inclusion threshold was set at 0.20.
- As regards the modelling procedure, the bottom-up step-by-step method was adapted: starting with the empty model, we added, one by one, variables that were significant in the univariate analysis. When moving from one model to the next, the WALD test was used to assess the significance of the variable introduced. When a variable was significant at a 5% threshold, it was retained in the model and the next variable was introduced. Otherwise, the variable was removed from the model.
The overall fit of the model was assessed using Lemeshow's goodness-of-fit test. The final model was considered to have a good fit when the goodness-of-fit p-value is >0.10.
Ethical considerations
Demographic and Health Surveys are subject to review by national ethics committees. Anonymity and confidentiality were respected during primary data collection. Written informed consent was submitted and accepted by participants prior to the start of data collection.
An authorization request was made and obtained online via the DHS platform (https://dhsprogram.com) from the DHS database management program (DHS-Program).
RESULTS
Socio-demographic characteristics
Of the 3,880 participants, over a third (38.6%) were in the 25-34 age group and over two-thirds (79%) had not attended school. Two-thirds (66.3%) had a job at the time of the interview, and 70% lived in rural areas. The findings also show that only 8.9% of participants were using a modern method of contraception. Lastly, almost half (47.8%) of the participants said the distance to reach the health facility was a major problem to them (Table 2).
Variables
Number(N=3880)
Percentages
Woman’s age (years)
15-24
907
24.0
25-34
1496
38.6
35-49
1477
37.4
Woman's education level
None
3072
78.7
Primary
392
10.1
Secondary/superior
416
11.2
Husband's education level
None
2786
71.8
Primary
297
7.7
Secondary/higher
754
20.5
Number of children under 5 per woman
< 3>
3012
77.6
≥ 3 children
868
22.4
Women's working status
No (with no job)
1366
33.7
Yes (with a job)
2514
66.3
Husband's occupation
No occupation
354
8.7
Public/private service
769
20.5
Tradeswoman/workwoman?
2673
70.8
Number of ANCs performed
< 4>
1753
45.5
≥4 ANCs
2127
54.5
Postnatal visit
No
332
25.5
Yes
937
74.5
Is the woman currently using a contraceptive method?
No
3559
91.1
Yes
321
8.9
Distance from health facility
A real problem
1890
47.8
Not a problem
1990
52.2
Woman’s socio-economic status
Poorest
895
22.5
Poorer
851
22.5
Middle
756
19.8
Richer
766
18.6
Richest
612
16.6
Place of residence
Urban
1142
29.1
Rural
2738
70.9
Region
Boké
584
11.4
Conakry
373
12.6
Faranah
486
9.9
Kankan
496
14.6
Kindia
505
14.8
Labé
483
11.8
Mamou
469
9.5
Nzérékoré
484
15.4
Table 2: Socio-demographic characteristics of participant’s
Prevalence of women's autonomy in healthcare decision-making
The prevalence of women's autonomy in healthcare decision-making in our sample was 10.3% (CI: 8.89-11.77), that is, 1 out of 10 women surveyed. This autonomy in decision-making increased with age, rising from 6.1% among adolescents and young people (15-24 years) to 14.1% among women in the 35-49 age group (P<0 p=0.009)>
Variables
Women's autonomy in healthcare decision-making
N(%) n =368
95% CI
P(value)
Woman’s age (years)
15-24
53 (6.1)
4.49 – 8.22
(<0>
25-34
127 (9.1)
7.38 – 11.14
35-49
188 (14.1)
11.87– 16.79
Woman's education level
None
281 (9.9)
8.37 – 11.60
0.435
Primary
38 (10.9)
7.45 – 15.75
Secondary/higher
49(12.3)
9.10 – 16.36
Husband's education level
None
271 (10.3)
8.73 – 12.07
0.870
Primary
25 (10.7)
7.01 – 15.90
Secondary/higher
65 (9.6)
7.18 - 12.62
Number of children under 5 years old
< 3>
283 (10.6)
8.99 – 12.37
0.333
≥ 3 children
85 (9.1)
7.02 – 11.78
Women's working status
No (with no job)
84 (6.4)
5.03 – 8.17
(<0>
Yes (with a job)
284 (12.2)
10.40 – 14.23
Husband’s occupation
No occupation
53 (15.9)
11.89 – 20.91
P = 0.002
Public/private service
74 (10.8)
8.08 – 14.30
Commerçante/ouvrière
217 (8.6)
7.25 – 10.24
Tradeswoman/workwoman
Number of ANCs performed
< 4>
139 (8.7)
6.81 – 11.13
0.048
≥4 ANCs
229 (11.5)
9.85 – 13.40
Distance from health facility
A real problem
183 (10.2)
8.43 – 12.20
0.919
Not a problem
185 (10.3)
8.36 – 11.43
Place of residence
Urban
134 (13.2)
10.61 – 16.32
0.009
Rural
234 (9)
7.49 – 10.84
Overall
368 (10.3)
8.89 – 11.77
Table 3: Prevalence of women's autonomy in healthcare decision-making by characteristics
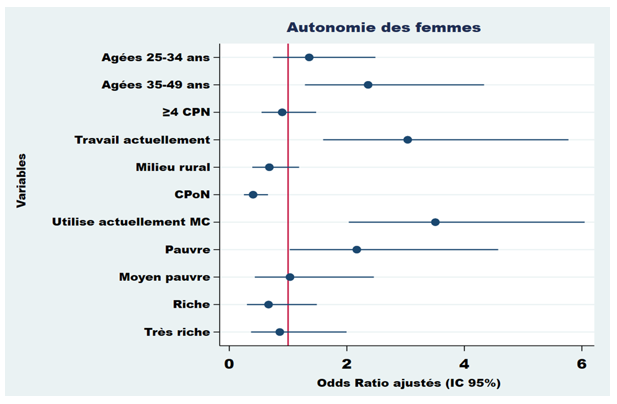
As shown in graph1 of the multivariate logistic regression model, variables such as age, current employment status, current use of a contraceptive method and socio-economic status were significantly associated with women's autonomy in healthcare decision-making in both univariate and multivariate analyses.
Women aged 35-49 were 2.36 times more likely to be autonomous in making decisions about their healthcare compared with those aged 15-24 AOR=2.36 (1.29 - 4.41), holding all other variables constant in the model. Similarly, the risk of being autonomous in making healthcare decisions was 3.035 times higher among working women compared with non-working women AOR= 3.035 (1.59 - 5.77). Also holding all other variables constant in the model, the probability of being autonomous in health care decision making was about 4 times higher among women who were currently using a contraceptive method compared to their counterpart who were not on a contraceptive method AOR= 3.51 (2.03 - 6.04). Women who had attended a postnatal consultation were 60% less likely to be autonomous in making decisions about their health care compared with those who did not attend a postnatal consultation AOR = 0.40 (0.25 - 0.69 (Graph 1).
Graph1: Graphical representation of factors associated with women's autonomy in healthcare decision-making in multivariate analysis
DISCUSSION
In many developing countries, particularly in sub-Saharan Africa, the vast majority of women are excluded from all decision-making processes concerning their own lives [19,20]. In Guinea, as in most of these countries, women's decision-making autonomy is an integral part of family well-being, particularly in terms of improving maternal and neonatal health.
The results of this study show that in Guinea, only a minority of women can make the decision to use a health service on their own. Barely one tenth of Guinean women (10.3%) are free to decide to use a health service without the consent of a third party. However, this result is higher than those for Senegal and Nigeria (6.2% and 6.26% respectively) [20,21].
The proportion of autonomy reported in this study was lower than that reported in a systematic review conducted in 2022 (55.16%) and in south-eastern Ethiopia (41.4%) [22,6]. This difference can be explained, on the one hand, by gender inequality, which places women in a position of inferiority in certain African communities, and, on the other hand, to the fact that efforts to empower women may vary from one country to another [23]. To a greater extent, maternal and child health is inherent to the level of empowerment exercised by women, as empowered women can make good choices and access quality health care at all times, particularly during antenatal consultations and labour [21].
The factors associated with women's autonomy in the present study were age, women's current working status, current use of a contraceptive method and socio-economic status. Women aged 35-49 were 2.36 times more likely to make a decision about their own healthcare than women aged 15-24 AOR = 2.36 (95% CI: 1.29 - 4.34). This could be due to the fact that the older a woman gets, the more mature she becomes and the more capable she is of becoming autonomous in all matters relating to her healthcare.
This result corroborates with that of a study conducted in Ethiopia, which also reported that the chance of being autonomous in decision-making was higher among women aged 30 and over than among women aged under 20 [19].
Nowadays, working status seems to be one of the crucial factors in the gender-role gap in the community in terms of healthcare-seeking behaviour, economic well-being and women's empowerment [5]. The results of this study showed that the probability of making a healthcare decision was 3 times higher among women with a job than those with no job (AOR= 3.04; 95% CI: 1.59 - 5.77). These results confirm those of studies conducted in Ethiopia, in Ghana, which reported that women with a job are more likely to make a decision about their own healthcare than women with no job [22,23]. This may be due to the fact that women with a job are generally better educated and better informed about life realities; their education and information levels thereby improve their self-confidence in making healthcare decisions while challenging beliefs of male dominance in society [23]. However, findings of studies in Ethiopia and South Africa found no association between women's decision-making autonomy in terms of healthcare and women's working status [24,25].
The findings show that the use of a contraceptive method was significantly associated with women's autonomy in terms of healthcare. Women using a contraceptive method had 3.51 times more power to decide about their own healthcare than their counterparts not using a contraceptive method [23]. These results are consistent with those reported in in Senegal, and in Ethiopia which found an association between the use of contraceptive methods and women's autonomy in terms of healthcare. A possible explanation for this finding is that women exposed to family planning information may have a better understanding of reproductive health rights and the benefits of contraceptives, which could encourage their participation in reproductive health decision-making [20,26].
In addition, this study showed that women from poor households were 2.17 times more likely to make a decision about their health status than women from rich households (AOR= 2.17: 1.02 - 4.57). Furthermore, contrary to previous studies our results showed that women from poor households were 2.17 times more likely to make decisions about their own health than women from rich households (AOR= 2.17: 1.02 - 4.57) [30,5]. These results are consistent with those reported in Ethiopia in 2012 [27]. This finding could be explained by the fact that women from wealthy households often lack self-esteem, which highlights their economic dependence on their families [27]. Women with low socio-economic status also have access to healthcare and are informed about the importance of their consent in healthcare decision-making.
Strengths and limitations
The main strength of the study was that it used nationally representative survey data with a large sample size. However, the data used in this study is cross-sectional, which limits conclusions about the causality of factors with the dependent variable. In addition, DHS is based on self-reported information, which is likely to be subject to social desirability bias due to its socio-cultural nature.
Implications for research and practice
This research has been instructive in describing some of the important factors in women's rights with respect to their empowerment. These findings are relevant to the development of strategies to strengthen women's role in addressing gender inequalities.
The study showed the need for greater involvement of women in decision-making about the use of healthcare, as well as the need for changes in national policies and guidelines to promote women's empowerment.
Improving married women's knowledge about the use of maternal and child health services in general, and about their sexual and reproductive lives in particular, is an important step in reducing maternal and child mortality.
CONCLUSION
Despite the fact that every woman has the right to make her own decisions about her own healthcare, only 10.3% of Guinean women played a role in decisions about healthcare use. Government authorities, with the support of stakeholders, should promote women's autonomy over their use of healthcare as an essential component of their sexual and reproductive health rights through education and the media, with a particular focus on adolescent girls, young people and adult women in general. It's about calling into question traditional male domination of decision-making within the household.
Acknowledgements
We are grateful for the support of the Guinea National Institute of Statistics in obtaining the database and for their valuable contributions to the collection of DHS data.
Financing: this study received financial support from the Guinean government for data collection through the National Institute of Statistics
Abbreviations GAVFSN: Global Analysis of Vulnerability, Food Security and Nutrition, ANC: Antenatal Consultation, DHS: Demographic and Health Survey, CI: Confidence Interval, OR: Odds Ratio, WHO: World Health Organization, NIS: National Institute of Statistics
Availability of data and materials Data from the Guinea Demographic and Health Survey (DHS) generated and/or analysed in the course of this study are available and accessible on the DHS Programme website (http://dhsprogram.com).
Ethical approval and consent to participate Ethical approval is not required for this study as it is a secondary analysis of the data and is available in the public domain. More details regarding DHS data and ethical standards can be found at: http://dhsprogram.com/data/available-datasets.cfm. This study does not have a participation section (secondary data analysis), so it is not applicable
Competing interests The authors declare that they have no competing interests.
Authors' contributions: MDB, AOS and MT participated in designing the study, MT contributed to the data analysis. All authors contributed to the interpretation of the data, drafting of the manuscript and review of the article. All authors contributed to the development, revision and approval of the final manuscript
References
World Health Organization, UNICEF, UNFPA, World Bank Group & and the United Nations Population Division (2019). Trends in maternal mortality 2000 to 2017 estimates by WHO, UNICEF,.pdf.. View
at PublisherView
at Google Scholar
Institut National de la Statistique, Ministère du Plan et du, & Développement Economique. Enquête Démographique et de Santé Guinée (2018). Institut National des Statistiques (INS) 650. View
at PublisherView
at Google Scholar
Kebede, A. A. et al (2021). Married women’s decision-making autonomy in the household and maternal and neonatal healthcare utilization and associated factors in Debretabor, northwest Ethiopia. PLoS ONE 16. View
at PublisherView
at Google Scholar
Sialubanje, C., Massar, K., Hamer, D. H. & Ruiter, R. A (2015). Reasons for home delivery and use of traditional birth attendants in rural Zambia: a qualitative study. BMC Pregnancy Childbirth 15, 216. View
at PublisherView
at Google Scholar
Aragaw, F. M. et al (2023). Individual and community level predictors of women’s autonomy in health care decision-making among youth in East African countries: a multilevel analysis. BMJ Open 13, e066975. View
at PublisherView
at Google Scholar
Nigatu, D., Gebremariam, A., Abera, M., Setegn, T. & Deribe, K (2014). Factors associated with women’s autonomy regarding maternal and child health care utilization in Bale Zone: a community based cross-sectional study. BMC Women’s Health 14, 79. View
at PublisherView
at Google Scholar
Acharya, D. R., Bell, J. S., Simkhada, P., van Teijlingen, E. R. & Regmi, P. R (2010). Women’s autonomy in household decision-making: a demographic study in Nepal. Reproductive Health 7, 15. View
at PublisherView
at Google Scholar
Ganle, J. K. et al (2015). How intra-familial decision-making affects women’s access to, and use of maternal healthcare services in Ghana: a qualitative study. BMC Pregnancy Childbirth 15, 1–17. View
at PublisherView
at Google Scholar
Sharma, S., Rao, P. K. & Sharma, R (2013). Role of Women in Decision-making Related to Farm: A study of Jammu district of J&K State. 3,. View
at PublisherView
at Google Scholar
Osamor, P. E. & Grady, C (2016). Women’s autonomy in health care decision-making in developing countries: a synthesis of the literature. Int J Womens Health 8, 191–202. View
at PublisherView
at Google Scholar
Gee, R. E. & Corry, M. P (2012). Patient engagement and shared decision making in maternity care. Obstet Gynecol 120, 995–997. View
at PublisherView
at Google Scholar
Asweto, C. O., Aluoch, J. R., Obonyo, C. O. & Ouma, J. O (2014). Maternal Autonomy, Distance to Health Care Facility and ANC Attendance Findings from Madiany Division of Siaya County, Kenya. View
at PublisherView
at Google Scholar
Asabu, M. D. & Altaseb, D. K (2021). The trends of women’s autonomy in health care decision making and associated factors in Ethiopia: evidence from 2005, 2011 and 2016 DHS data. BMC Women’s Health 21, 371. View
at PublisherView
at Google Scholar
Merrell, L. K. & Blackstone, S. R (2020). Women’s Empowerment as a Mitigating Factor for Improved Antenatal Care Quality despite Impact of 2014 Ebola Outbreak in Guinea. Int J Environ Res Public Health 17, 8172. View
at PublisherView
at Google Scholar
Ministère de l’Agriculture, Guinée (2018). Analyse Globale de La Vulnérabilité, de La Sécurité Alimentaire et de La Nutrition (AGVSAN). 170. View
at PublisherView
at Google Scholar
Conceição, P. C (2021). DÉVELOPPEMENT HUMAIN: Temps incertains, vies bouleversées : façonner notre avenir dans un monde en mutation. View
at PublisherView
at Google Scholar
Alemayehu, M. & Meskele, M (2017). Health care decision making autonomy of women from rural districts of Southern Ethiopia: a community based cross-sectional study. Int J Womens Health 9, 213–221 View
at PublisherView
at Google Scholar
Sougou, N. M., Bassoum, O., Faye, A. & Leye, M. M. M (2020). Women’s autonomy in health decision-making and its effect on access to family planning services in Senegal in 2017: a propensity score analysis. BMC Public Health 20, 872. View
at PublisherView
at Google Scholar
Odusina, E. K. & Oladele, O. S (2023). Is there a link between the autonomy of women and maternal healthcare utilization in Nigeria? A cross-sectional survey. BMC Women’s Health 23, 167. View
at PublisherView
at Google Scholar
Tesema, G. A. et al (2021). Spatial clusters distribution and modelling of health care autonomy among reproductive‐age women in Ethiopia: spatial and mixed‐effect logistic regression analysis. BMC Health Services Research 21, 74. View
at PublisherView
at Google Scholar
Duah, H. & Adisah, A (2017). Determining health care decision making autonomy among mothers of children under five years in Ghana: analysis of 2014 Ghana demographic and health survey, View
at PublisherView
at Google Scholar
Edossa, Z. K., Debela, T. F. & Mizana, B. A (2020). Women’s Decision on Contraceptive Use in Ethiopia: Multinomial Analysis of Evidence From Ethiopian Demographic and Health Survey. Health Serv Res Manag Epidemiol 7, 2333392820924565. View
at PublisherView
at Google Scholar
Osuafor, G. N., Maputle, S. M. & Ayiga, N (2018). Factors related to married or cohabiting women’s decision to use modern contraceptive methods in Mahikeng, South Africa. Afr J Prim Health Care Fam Med 10, 1431. View
at PublisherView
at Google Scholar
Mare, K. U., Aychiluhm, S. B., Tadesse, A. W. & Abdu, M (2022). Married women’s decision-making autonomy on contraceptive use and its associated factors in Ethiopia: A multilevel analysis of 2016 demographic and health survey. SAGE Open Med 10, 20503121211068719. View
at PublisherView
at Google Scholar
Asabu, M. D. & Altaseb, D. K (2021). The trends of women’s autonomy in health care decision making and associated factors in Ethiopia: evidence from 2005, 2011 and 2016 DHS data. BMC Women’s Health 21, 371. View
at PublisherView
at Google Scholar
"ScienceHood Publishing exceeded our expectations with their seamless execution and professionalism. Their team ensured timely communication, high-quality production, and attention to detail throughout the process. They transformed our vision into reality, delivering exceptional results. We highly recommend them for their efficiency, expertise, and commitment to excellence in publishing."
Lara Simmons
"ScienceHood Publishing surpassed our expectations with their professionalism, timely communication, and exceptional attention to detail. They transformed our vision into reality with outstanding results. We highly recommend them for their expertise and commitment to excellence."
Shippora Smith
"Publishing in this journal gave me the opportunity to involve Bioinformatics, which is a cutting-edge field with so much potential, into my previous research on Optogenetics and Artificial Intelligence. This experience helped me better understand how closely interconnected STEM fields truly are, and how many opportunities exist for interdisciplinary collaboration to allow them to work together and, once again, change the world, as science has always done"
Tomas Hadi Acosta Aguilera
"Dear editors,
It has also been a real pleasure working with you on the publication of our article. Your patience, understanding, and prompt responses whenever we needed them have been a great help to us in this joint endeavour."


 :
© 2025 Madeleine TOURE. This open-access article is distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
:
© 2025 Madeleine TOURE. This open-access article is distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.