Abstract
Background
Sphenoid sinusitis is a relatively uncommon finding that typically presents with headaches, head fullness, and chronic cough. Cranial nerve involvement is rare, and isolated trochlear nerve palsy is distinctly unusual.
Description of Case
We describe a 56-year-old man who presented with subtle diplopia and was found to have a left fourth nerve palsy. CT and MRI of the brain revealed sphenoid sinus infection compatible with a mycetoma. A potential causal link between the lesion and the cranial neuropathy remained uncertain. Antibiotic and steroid therapy resulted in no clinical or imaging improvement, and the patient underwent uncomplicated functional endoscopic sphenoid sinusotomy with removal of the lesion. At the time of three-month follow-up, the fourth nerve palsy had improved considerably.
Conclusions
The postoperative improvement in this case highlights the potential reversibility of cranial nerve dysfunction in the setting of sphenoid sinus infection, even when chronic in nature. We suggest that surgery should be considered in such cases.
INTRODUCTION
Sphenoid sinusitis represents less than 3% of all sinus infections [1]. Typical clinical presentation includes headache, nasal discharge, chronic cough, and a sense of head fullness [1]. Cranial neuropathy has been reported rarely in this setting [2]. We describe a patient who presented with an isolated fourth nerve palsy which improved significantly after endoscopic surgical removal of a chronic sphenoid sinus infection. This report highlights the reversibility of cranial neuropathy even in the face of chronic, long-standing infection of the sphenoid sinus.
CASE PRESENTATION
A 56-year-old surgeon with a long history of migraine headaches presented to a neuro-ophthalmologist with the complaint of subtle diplopia over an eighteen-month period. This was exacerbated by fatigue and noted while working under the operating microscope. Neuro-ophthalmological evaluation revealed briskly reactive pupils without an afferent pupillary defect. Extraocular motility was full in each eye. There was no evidence of ptosis. Alternate cover testing showed a 1-prism diopter intermittent left hypertropia in primary gaze that increased to 2-prism diopters in right gaze and left head tilt. It improved to a minimal intermittent left hypertropia in left gaze and right head tilt. This was confirmed with single Maddox rod. The patient was diagnosed with a left fourth nerve palsy and given a 2 base-down Fresnel prism on the left lens.
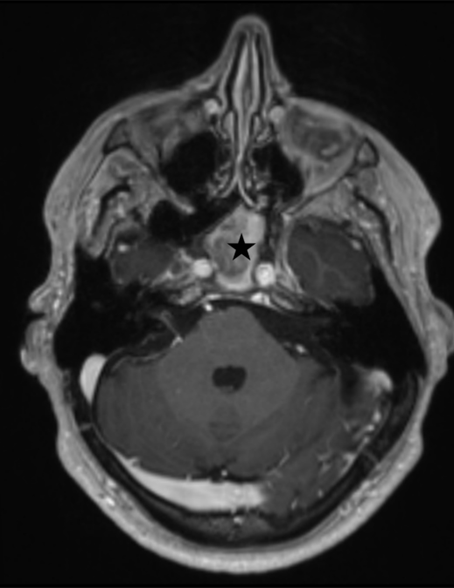
Brain MR imaging with and without contrast revealed significant sphenoid sinusitis with chronic inflammatory changes involving the adjacent clivus and areas of magnetic susceptibility raising the possibility of a superimposed fungal infection.
Figure 1. T-1 weighted axial MR image with intravenous gadolinium contrast showing the sphenoid sinus filled with high signal intensity, presumed infectious material (black star).
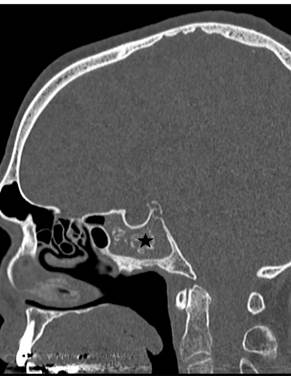
(Figure 1) After consultation with an otolaryngologist, a trial of prednisone and antibiotics was instituted with no change in symptoms. A follow-up CT scan showed no change in the sphenoid sinus lesion but also revealed intralesional calcification further supporting the diagnosis of mycetoma.
Figure 2. Axial (A) and sagittal (B) CT images showing calcified material (black stars) filling the sphenoid sinus suggesting the diagnosis of mycetoma.
Figure 2. Axial (A) and sagittal (B) CT images showing calcified material (black stars) filling the sphenoid sinus suggesting the diagnosis of mycetoma.
(Figure 2) It was unclear whether the isolated fourth nerve palsy was related to the sphenoid sinus infection.
The patient chose to undergo functional endoscopic sphenoid sinus surgery. At the time of surgery, multiple pieces of thick and partially calcified tissued were removed from the sphenoid sinus and submitted for histopathologic evaluation, gram stain, and culture. The procedure was uneventful, and the final diagnosis was mycetoma. Gram stain was negative, and final cultures were unremarkable. The patient tolerated the procedure well without complication. At the time of three-month neuro-ophthalmology follow-up, the fourth nerve palsy had significantly improved. Although it was felt by the ophthalmologist that a prism was no longer necessary, the patient still noted benefit from a 1 base-down Fresnel prism on the left lens. Further follow-up is scheduled at the one-year mark.
DISCUSSION
Sphenoid sinusitis typically presents with headache, head fullness, and chronic cough [1]. Chronic inflammation with superimposed fungal infection may occur, and endoscopic sinus surgery is typically required in such cases [3-5]. The development of cranial neuropathy most typically affecting vision itself has been described in rare cases [6-8]. In these instances, involvement of the optic nerve resulting in vision loss or dysfunction of the oculomotor or abducens nerve have been reported most commonly. Trochlear nerve palsy, as described in our report, is extremely rare [9-11].
Kim et al reported 47 patients with sphenoid sinus mycetoma. The most common complaints were nasal symptoms in 27 and headache in 26; eight patients had impaired visual acuity, and five of these had extraocular movement restriction. After treatment, visual acuity improved in 2, and extraocular movement in 2.
The proximity of the sphenoid sinus to major neurovascular structures provides a clear explanation for the risk of cranial nerve involvement in this setting [2]. The trochlear nerve (cranial nerve IV) courses along the lateral wall of the cavernous sinus, immediately adjacent to the sphenoid sinus, and can therefore be affected by expanding lesions such as a mycetoma [13]. In cases of non-invasive fungal infection, the mechanism is likely related to local inflammatory edema or mass effect rather than direct invasion [4,14]. These processes may irritate the nerve sheath or compromise vascular supply, leading to neuropathy [14]. This differs from more aggressive fungal infections, where direct tissue destruction is typical, but illustrates how even chronic, non-invasive lesions can still produce cranial nerve dysfunction that can be reversed when pressure is relieved through surgical decompression [3,6].
Reports of isolated trochlear nerve palsy due to sphenoid sinus disease are exceedingly unusual [11,15]. Most cases of cranial neuropathy in this context involve the abducens (VI) or oculomotor (III) nerves, often in combination, while trochlear involvement is more commonly seen as part of broader processes such as orbital apex syndrome or pansinusitis, as seen in one reported case involving cranial nerves III, IV, and VI [9,10,15]. Isolated trochlear palsy from a sphenoid mycetoma has been described only in a few instances, with most similar cases instead attributed to mucoceles or inflammatory spread from adjacent sinuses [15]. Importantly, the literature suggests that up to 82% of cranial neuropathies may improve following timely surgical intervention, even when the infection is long-standing [15]. This underscores the importance of considering early surgical decompression to prevent the development of irreversible deficits [12,6].
Although improvement in cranial neuropathy following treatment is unpredictable, the potential for such improvement has been emphasized in the past [12]. In large studies, the most common causes of isolated trochlear nerve palsy in adults include trauma, microvascular disease, and decompensation of a congenital palsy [16-17]. In the present case, decompensation of a long-standing trochlear palsy was considered as a possible etiology. Because the causal relationship between the sphenoid sinus infection and fourth nerve dysfunction was uncertain, it was challenging to predict the likelihood of improvement with treatment. Ultimately, there was meaningful improvement in the fourth nerve function, strongly suggesting that the mycetoma had resulted in local inflammation and irritation causing the neuropathy. Despite the chronic nature of the infection as well as the fourth nerve dysfunction, the improvement in our case suggests that even chronic lesions can improve with surgical treatment.
CONCLUSION
Although rare, sphenoid sinus infection can result in irritation of multiple cranial nerves. Despite the fact that the infection may be long-standing, the present case highlights the potential reversibility of such cranial neuropathy with surgical decompression of the sphenoid sinus. Patients with extra-ocular impairment due to cranial neuropathy in the setting of sphenoid sinus infection should be considered for surgical decompression.
Disclosures
The authors report no conflicts of interest.
Patient permission was obtained, and IRB approval was granted for the current study.
References
-
Lew D, Southwick FS, Montgomery WW, Weber AL, Baker AS. Sphenoid sinusitis: a review of 30 cases. N Engl J Med. 1983 Nov;309(19):1149–1154.
View
at Publisher
View
at Google Scholar
-
Lawson W, Reino AJ. Isolated sphenoid sinus disease: an analysis of 132 cases. Laryngoscope. 1997 Dec;107(12 Pt 1):1590-1595.
View
at Publisher
View
at Google Scholar
-
deShazo RD, Chapin K, Swain RE. Fungal sinusitis. N Engl J Med. 1997 Jul;337(4):254–259.
View
at Publisher
View
at Google Scholar
-
Ferguson BJ. Fungus balls of the paranasal sinuses. Otolaryngol Clin North Am. 2000 Apr;33(2):389–398.
View
at Publisher
View
at Google Scholar
-
Klossek JM, Serrano E, Peloquin L, Percodani J, Fontanel JP, Pessey JJ. Functional endoscopic sinus surgery and 109 mycetomas of paranasal sinuses. Laryngoscope. 1997 Jan;107(1):112–117.
View
at Publisher
View
at Google Scholar
-
Postma GN, Chole RA, Nemzek WR. Reversible blindness secondary to acute sphenoid sinusitis. Otolaryngol Head Neck Surg. 1995 Jun;112(6):742–746.
View
at Publisher
View
at Google Scholar
-
Hu L, Wang D, Yu H. Isolated sphenoid fungal sinusitis and vision loss: the case for early intervention. J Laryngol Otol. 2009 Feb;123(2):e8.
View
at Publisher
View
at Google Scholar
-
Lee LA, Huang CC, Lee TJ. Prolonged visual disturbance secondary to isolated sphenoid sinus disease. Laryngoscope. 2004 Jun;114(6):986–990.
View
at Publisher
View
at Google Scholar
-
Ada M, Kaytaz A, Tuskan K, Güvenç MG, Selçuk H. Isolated sphenoid sinusitis presenting with unilateral VIth nerve palsy. Int J Pediatr Otorhinolaryngol. 2004 Apr;68(4):507-510.
View
at Publisher
View
at Google Scholar
-
Gupta R, Shukla R, Mishra A, Parihar A. Isolated acute sphenoid sinusitis presenting with hemicranial headache and ipsilateral abducens nerve palsy. BMJ Case Rep. 2015 Jun 8;2015:bcr2015209408.
View
at Publisher
View
at Google Scholar
-
Chen, L., Jiang, L., Yang, B. et al. Clinical features of visual disturbances secondary to isolated sphenoid sinus inflammatory diseases. BMC Ophthalmol 17, 237 (2017).
View
at Publisher
View
at Google Scholar
-
Kim JS, Kim BK, Hong SD, Kim HJ, Kim HY. Clinical Characteristics of Sphenoid Sinus Fungal Ball Patients With Visual Disturbance. Clin Exp Otorhinolaryngol. 2016 Dec;9(4):326-331.
View
at Publisher
View
at Google Scholar
-
Jumper N, Unger K. Neuroanatomy, Cranial Nerve 4 (Trochlear). In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
View
at Publisher
View
at Google Scholar
-
Alsaleh MA, Almomen AA. Abducens nerve palsy secondary to allergic fungal sinusitis. J Surg Case Rep. 2024 Nov 16;2024(11):rjae697.
View
at Publisher
View
at Google Scholar
-
El Mograbi A, Soudry E. Ocular cranial nerve palsies secondary to sphenoid sinusitis. World J Otorhinolaryngol Head Neck Surg. 2017 Mar 6;3(1):49-53.
View
at Publisher
View
at Google Scholar
-
Keane JR. Fourth nerve palsy: historical review and study of 215 in patients. Neurology. 1993;43:2439–2443.
View
at Publisher
View
at Google Scholar
-
Dosunmu EO, Hatt SR, Leske DA, Hodge DO, Holmes JM. Incidence and Etiology of Presumed Fourth Cranial Nerve Palsy: A Population-based Study. Am J Ophthalmol. 2018 Jan;185:110-114
View
at Publisher
View
at Google Scholar
-
Oh SY. Clinical outcomes and aetiology of fourth cranial nerve palsy with acute vertical diplopia in adults. Eye (Lond). 2020 Oct;34(10):1842-1847.
View
at Publisher
View
at Google Scholar


 :
© 2025 Eric S. Nussbaum. This open-access article is distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
:
© 2025 Eric S. Nussbaum. This open-access article is distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.